
Introduction to pediatric RMST
Respiratory muscle training (RMST) is an effective therapy to reverse the clinical condition of respiratory muscle weakness (RMW). RMW is prevalent in people with respiratory, cardiac and neuromuscular disease, and during healthy aging. Symptoms of RMW include dyspnea, limited exercise tolerance, and reduced quality of life.
RMW however is not limited to adults. Children and young people with respiratory diseases such as asthma, chronic lung disease or cystic fibrosis, as well as those with neuromuscular disease and cardiac conditions are affected by RMW. Improving respiratory muscle strength by RMST is an effective therapeutic method to help children and young people with RMW.
Clinical benefits of RMST in infants, children and young people:
- Improved respiratory muscle strength (MIP, MEP)
- Improved peripheral muscle strength and cardiorespiratory fitness (maximum strength, VO2max)
- Improved ventilatory efficiency (VE/VCO2 slope)
Improved peak cough flow and peak expiratory flow (PCF, PEF) - Improved respiratory rate
- Improved tidal volume (Vt)
- Increased success of liberation from mechanical ventilation in infants
- Reduced frequency of asthma exacerbations
- Improved ability to perform ADL (Activities of Daily Living)
- Reduced diurnal and nocturnal symptoms of asthma
- Reduced use of rescue bronchodilator
Specific considerations for pediatric RMST:
RMST in children and young people needs to be specifically tailored to age, weight, capacity, and disease status for optimal benefit and to avoid respiratory muscle overexertion. In addition, the RMST device and mouthpiece must suit the distinct features of children and young people to support correct handling, close lip seal and appropriate breathing technique.
Development of muscle strength
Children and young people have lower respiratory muscle strength, which correlate with their sex, age and/or weight [1–3]. During adolescence, respiratory muscle strength approaches adult values, with expiratory muscle strength lagging behind the rapid increase in inspiratory muscle strength [2].
Table 1 shows a comparison of average MIP/MEP values for adults and children aged 11.
Table 1: Obtained normal values for MIP and MEP (in cmH2O):

The right training protocol for pediatric RMST
Children and young people should train at a slightly lower intensity than adults. Target RMST intensity is 30% to 50% of MIP/MEP. Training protocols need to be adjusted according to disease. RMST sessions of 10 to 20 minutes with rest every 1 to 3 minutes on 5 to 6 days per week have proven effective. RMST should be maintained for at least 4 weeks [4–6].
Recommended RMST protocol: Daily sessions of 20 minutes of RMST. 1 minute of RMST should be followed by 1 minute of rest. Optimal RMST training intensity is around 40% of MIP. The patient should therefore be able to finish the one minute set of RMST without much difficulty (some noticeable effort).
Estimating respiratory muscle strength in children
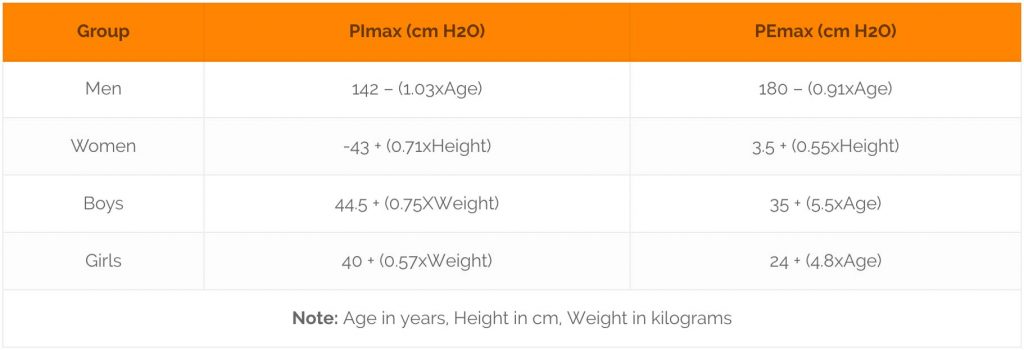
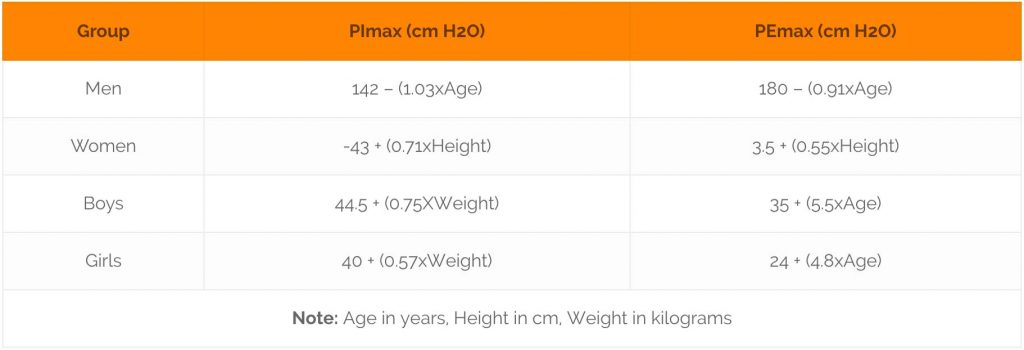
If measurements of the maximum respiratory pressures can not be obtained, these can be approximated according to the following equations derived from empirical data [1].
Table 2: Equations to calculate MIP and MEP
Evidence for the impact of pediatric RMST
Several clinical studies provide evidence for the effectiveness of RMST in children and young people.
- A study including 29 children and young people aged 5 to 17 years, who suffered from chronic lung disease (CLD) or neuromuscular disease (NMD) evaluated the impact of 6 month of home-based RMST. Respiratory muscle strength (MIP, MEP), peak expiratory flow (PEF) and peak cough flow (PCF) were measured before and after RMST. While respiratory muscle strength increased in both patient groups, increases in PCF and PEF reached significance only in the NMD group, not in the CLD group.
- Improvements in NMD patients: MIP: +45%, MEP: +38%, PEF: +57%, PCF: +31%
- Improvements in CLD patients: MIP: +33%, MEP: +33%, PEF: +14%, PCF: +9%
These data are clinically meaningful, as it proves that RMST can slow and even temporarily reverse deterioration of lung function in children and young people with NMD and CLD [4].
- A group of 21 children and young people with NMD with an average age of 12 years underwent 6 months of RMST, with a 12 months follow up, and the results were compared to an age-and sex-matched control group. Respiratory muscle strength (MIP, MEP) and respiratory load perception (RLP) were evaluated every 3 months for one year. RLP assesses the perception of dyspnea at a fixed respiratory load (15 cm H2O).
- MIP and MEP significantly increased after 3 and 6 months of RMST, and returned to baseline values after 18 months.
- RLP significantly decreased after 6 months of RMST and remained low throughout follow up period.
This study confirms the feasibility and benefit of long-term RMST in children with progressive NMD. Long-term reduction of RLP will greatly improve comfort and health-related quality of life (QOL) in NMD patients [6].
- Children aged 8 to 12 years who suffer from asthma were treated with RMST for 7 weeks. Benefits of RMST were compared to a control group. During this time, they did two supervised sessions per week. Respiratory muscle strength, PEF and several asthma severity variables were assessed before and after RMST, including frequent asthma attacks; diurnal symptoms; nocturnal symptoms; impaired ability to perform activities of daily living; emergency room treatment; hospitalisation; and rescue bronchodilator use.
- RMST significantly improved MIP by 130%.
- RMST significantly improved MEP by 60%.
- RMST significantly improved PEF by 80%.
- IMST (inspiratory muscle strength training) further significantly reduced the frequency of asthma attacks, improved the ability to perform daily activities, reduced diurnal and nocturnal symptoms as well as the frequency of rescue bronchodilator use.
RMST, therefore, is a suitable and effective adjuvant therapy for children with asthma, as it improves respiratory muscle strength and cough function. RMST also reduces the severity of the disease, thus improving health-related QOL [5].
- The Fontan procedure is a specialist surgical method for children with only one functional cardiac ventricle or other congenital heart diseases, where one ventricle is bypassed and the systemic and pulmonary circulation are placed in series [7]. Children with Fontan circulation suffer from respiratory muscle weakness. RMST by inspiratory muscle training for 6 weeks with daily sessions of 30 mins significantly improved respiratory muscle strength and exercise capacity in 23 young adults (average age 16 years) with Fontan circulation.
- RMST significantly improved MIP by 46%.
- RMST significantly improved ventilatory efficiency of exercise.
- RMST significantly improved resting cardiac output and ejection fraction.
This study shows that RMST is an effective method to improve respiratory muscle strength, exercise capacity and cardiac function in young adults with Fontan circulation. RMST should, therefore, contribute to reducing morbidity and to increasing health-related QOL in these young people [8].
Small study of 10 children (10-11yrs) with cystic fibrosis (CF) using IMST in addition to aerobic and strength exercises. 8 week program followed by 4 weeks of detraining, significant improvements in PImax, VO2max and maximum strength. Abstract only.
29 children (avg 12 yrs) with NMD or CLD (including CF) did 6 months of IMST plus EMST. 30-50% of MIP/MEP, 3 x 3 min, 1 min rest, 5 days per week. Significant improvements in MIP, MEP, PCF, PEF. In the introduction they discuss other studies using RMST at 20-30% of MIP in children.
Two infant case studies (147 days and 112 days) with different case history but common mechanical ventilation, decline from baseline respiratory function and ventilatory muscle dysfunction underwent individually tailored IMST, 5-6 mornings per week, 8-12 inhalations against occlusion over 15 days and 7 days, respectively. Both showed improved MIP and time to reach MIP, respiratory rate and tidal volume. Both patients could be extubated and discharged.
Systematic review of RMST in children with NMD (5-18yrs). Significant improvement of MIP due to IMST, but amount of evidence too low for conclusions.
Study of average PImax and PEmax in children (girls and boys, 8 to 17 years). Average PImax: 112 cm H2O, PEmax: 143 cmH2O. Conclusion: PImax comparable to adult values, PEmax slightly lower. Very variable sample (27 girls, 13 boys of a wide age range).
Evaluation of PImax in 22 ventilated children (mean age: 4.5 yrs). PImax: 46 cmH2O.
The clinical outcomes peak expiratory flow (PEF), maximal inspiratory pressure (MIP), maximal expiratory pressure (MEP) and severity variables were measured in 50 children (8-12 yrs) with asthma before and after a 7 week IMST with breathing exercises, as well as after 90 days, and compared to a control group. IMST significantly improved MIP (By 130%!), MEP (by 60%) and PEF (by 80%). IMST further significantly reduced the frequency of asthma attacks, improved the ability to perform daily activities, reduced diurnal and nocturnal symptoms as well as the frequency of rescue bronchodilator use. Protocol: 1 min IMST, 1 min rest for 20 min, then 5 min continuous use, intensity: 40% of MIP.
6 months of IMST plus PEP in 41 patients with NMD (DMD or SMA type III, avg age: 12yrs) significantly improved MIP, MEP and respiratory load perception. Results were maintained long-term. Protocol: Using both devices: 1 min at lowest setting (start at 7cmH2O), 1 min rest, increase pressure by 2 cmH2O until they reached their targeted maximal training pressures (at least 30% of the Pimax or Pemax). 2x per day.
6 weeks of IMST in 23 adolescents (avg age 16) with Fontan circulation significantly improved MIP, Peak VO2, VE/VCO2 slope (ventilatory efficiency), resting cardiac output, stroke volume, ejection fraction. Protocol: 30 min per day at 30% of MIP.
References
- Wilson SH, Cooke NT, Edwards RH, Spiro SG. Predicted normal values for maximal respiratory pressures in caucasian adults and children. Thorax. 1984;39: 535–538.
- Wagener JS, Hibbert ME, Landau LI. Maximal respiratory pressures in children. Am Rev Respir Dis. 1984;129: 873–875.
- Harikumar G, Moxham J, Greenough A, Rafferty GF. Measurement of maximal inspiratory pressure in ventilated children. Pediatr Pulmonol. 2008;43: 1085–1091.
- Núñez IR, Araos DZ, Delgado CM. Effects of home-based respiratory muscle training in children and adolescents with chronic lung disease. J Bras Pneumol. 2014;40: 626–633.
- Lima EVCL, Lima WL, Nobre A, dos Santos AM, Brito LMO, Costa M do R da SR. Inspiratory muscle training and respiratory exercises in children with asthma. J Bras Pneumol. 2008;34: 552–558.
- Gozal D, Thiriet P. Respiratory muscle training in neuromuscular disease: long-term effects on strength and load perception. Med Sci Sports Exerc. 1999;31: 1522–1527.
- Gewillig M. The Fontan circulation. Heart. 2005;91: 839–846.
- Laohachai K, Winlaw D, Selvadurai H, Gnanappa GK, d’Udekem Y, Celermajer D, et al. Inspiratory Muscle Training Is Associated With Improved Inspiratory Muscle Strength, Resting Cardiac Output, and the Ventilatory Efficiency of Exercise in Patients With a Fontan Circulation. J Am Heart Assoc. 2017;6. doi:10.1161/JAHA.117.005750
- Santana-Sosa E, Gonzalez-Saiz L, Groeneveld IF, Villa-Asensi JR, Barrio Gómez de Aguero MI, Fleck SJ, et al. Benefits of combining inspiratory muscle with “whole muscle” training in children with cystic fibrosis: a randomised controlled trial. Br J Sports Med. 2014;48: 1513–1517.
- Bieli C, Summermatter S, Boutellier U, Moeller A. Respiratory muscle training improves respiratory muscle endurance but not exercise tolerance in children with cystic fibrosis. Pediatr Pulmonol. 2017;52: 331–336.
- Smith BK, Bleiweis MS, Neel CR, Martin AD. Inspiratory muscle strength training in infants with congenital heart disease and prolonged mechanical ventilation: a case report. Phys Ther. 2013;93: 229–236.
- Human A, Corten L, Jelsma J, Morrow B. Inspiratory muscle training for children and adolescents with neuromuscular diseases: A systematic review. Neuromuscul Disord. 2017;27: 503–517.
- Hautmann H, Hefele S, Schotten K, Huber RM. Maximal inspiratory mouth pressures (PIMAX) in healthy subjects–what is the lower limit of normal? Respir Med. 2000;94: 689–693.





